In our first edition of Survivor, we followed a typical group of 36 kids that were diagnosed on one day with childhood cancer. We used 36 kids because when the first article was written, in the United States, on average 36 were diagnosed each day of the year. Since I wrote the original Survivor article, the number has risen to 47 kids diagnosed per year. We “followed” the group of 36 for 30 years. Along the way, some died,  but about 80% survived and some of the survivors would later die in their 30’s, 40’s and 50’s because of something called a late-term side effect. There are slightly more than 500,000 childhood survivors alive in the United States today. Imagine 500,000 survivors of childhood cancer! In the fifties and sixties, the cure rate for just about any type of cancer in children was so terribly low that no one would have ever believed we could have that many survivors over the next fifty years. Isn’t that great progress? Unfortunately, the answer is a hesitant, “Yes.” Hesitant because, while it’s great to have so many people beat childhood cancer, it also brings a lot of questions as to how are we going to take care of nearly half a million people who we now know are virtual ticking time-bombs when it comes to their future catastrophic health issues. Yes, catastrophic health issues because the same treatment they received that saved them from cancer may suddenly end or alter their lives due to the late-term effect of the toxic chemicals and radiation their bodies absorbed as
but about 80% survived and some of the survivors would later die in their 30’s, 40’s and 50’s because of something called a late-term side effect. There are slightly more than 500,000 childhood survivors alive in the United States today. Imagine 500,000 survivors of childhood cancer! In the fifties and sixties, the cure rate for just about any type of cancer in children was so terribly low that no one would have ever believed we could have that many survivors over the next fifty years. Isn’t that great progress? Unfortunately, the answer is a hesitant, “Yes.” Hesitant because, while it’s great to have so many people beat childhood cancer, it also brings a lot of questions as to how are we going to take care of nearly half a million people who we now know are virtual ticking time-bombs when it comes to their future catastrophic health issues. Yes, catastrophic health issues because the same treatment they received that saved them from cancer may suddenly end or alter their lives due to the late-term effect of the toxic chemicals and radiation their bodies absorbed as  children.
children.
A study in the Annals of Internal Medicine found that many primary care doctors feel they’re not prepared to deal with adult survivors of childhood cancer. Most doctors said they felt a little uncomfortable caring for childhood cancer survivors. Most in the study said they preferred to care for childhood cancer survivors in tandem with a doctor at a cancer center. Special thanks needs to be given to the American Cancer Society (ACS). The ACS saw problems with childhood cancer survivors obtaining proper treatment later in life and published a  special report in “CA” a journal for clinicians. Using the ACS report, Childhood and Adolescent Cancer Statistics 2014, and other sources this 2nd Edition of Survivor will focus on a discussion of the long-term side effects that childhood cancer survivors will have to overcome with the help of their primary care physicians. It seems when you survive childhood cancer it’s not the end, it’s the beginning of surviving all over again.
special report in “CA” a journal for clinicians. Using the ACS report, Childhood and Adolescent Cancer Statistics 2014, and other sources this 2nd Edition of Survivor will focus on a discussion of the long-term side effects that childhood cancer survivors will have to overcome with the help of their primary care physicians. It seems when you survive childhood cancer it’s not the end, it’s the beginning of surviving all over again.
Nothing is certain when it comes to late effects, but children who get chemotherapy and/or radiation therapy also have a small, but definitely increased, risk of second cancers later in life. These cancers include bone cancer, leukemia, or other soft tissue tumors. The bone cancers seem to be linked with radiation therapy, while the leukemias are more often seen after treatment with cyclophosphamide and related drugs. Information is provided in the ACS report, but more detailed information for a particular type of cancer can be found on the American Cancer Society website.
Acute Lymphocytic Leukemia (ALL)**: Long-term adverse health effects among children treated for ALL include neurocognitive defects, growth deficiency, and an increased risk of second cancers such as AML or lymphoma. Early forms of Central Nervous System (CNS) prophylaxis (treatment) that combined high doses of radiation and intrathecal chemotherapy resulted in a high risk of neurocognitive defects; less-toxic therapies that avoid the use of radiation have reduced, but not eliminated, these risks. In addition, children treated with cranial radiation therapy (CRT) for ALL in the past had an increased risk of developing CNS and head and neck tumors. High-dose therapeutic radiation is a recognized cause of brain tumors. Children who receive cranial irradiation for ALL or other cancers have an excess risk of brain and CNS tumors. Radiation therapy is now used in only a small fraction of patients with ALL who are at high risk of CNS recurrence. Patients with ALL who are treated with anthracyclines are at risk for late cardiac effects.
Acute Myeloid Leukemia (AML)**: Treatment toxicity and long-term effects for patients with AML are similar to those for patients with ALL; however, AML less often requires treatment or prophylaxis of the CNS, and therefore side effects related to radiation of the brain are not as common. Improvements in survival for patients with AML are associated with the use of higher doses of anthracycline chemotherapy than were used in the past. A follow-up study of 5-year survivors of AML treated from 1970 through 1986 found a relatively low prevalence of cardiac disease; however, there is concern that the prevalence of anthracycline-related cardiac toxicity may increase in more contemporary patient cohorts treated with higher doses.
Hodgkin Lymphoma**: Depending on the treatment received, long-term and late effects of treatment can include pulmonary dysfunction, cardiac disease, thyroid abnormalities, infertility, and second malignant neoplasms. Girls aged 10 years and older and young women treated with radiation to the chest for HL have a high relative and absolute risk of breast cancer. One study estimated a cumulative risk of breast cancer of 10% by age 45 years for women treated with chest irradiation (greater than 40 grays [Gy]) for HL at age 15 years. Current guidelines recommend annual MRI as an adjunct to mammographic screening for women who were treated for HL.
Non Hodgkins Lymphoma**: Depending on the chemo drugs used, fertility (the ability to have children) can be affected. Nerve damage, causing numbness, tingling, or even pain in the hands and feet, can also occur. In rare cases, people may develop leukemia several years later.
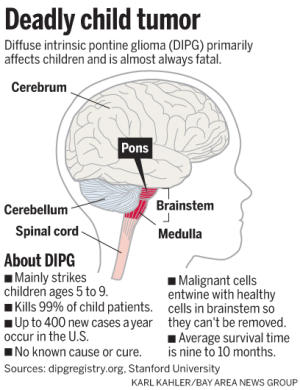
Brain Tumors (Ependymoma, Astrocytoma, Medulloblastomia)**: Survival rates  vary depending on tumor type, location, and grade. While there has been progress in survival for Central Nervous System (CNS) tumors overall, there has been little progress for some subtypes, such as diffuse intrinsic pontine glioma (DIPG), for which the median survival time after diagnosis remains less than one year. Improvements in survival for many types of CNS malignancies have resulted from advances in neurosurgical techniques, delivery of radiation therapy, supportive care, and use of combination chemotherapy. Nevertheless, children treated for brain tumors have a high risk of long-term morbidity and mortality. Late neurologic complications observed in follow-up studies of 5-year survivors include new onset of seizures, weakness in the arms and legs, blindness, and hearing loss. Children who receive radiation therapy to the hypothalamic-pituitary axis often experience neuroendocrine effects, including growth hormone deficiency, hypothyroidism, and abnormal timing of menarche. Cranial radiation therapy, particularly when used in very young children, can also result in neurocognitive deficits. For this reason, treatment protocols for patients with CNS tumors have been modified so that children aged younger than 3 years usually receive chemotherapy first with delayed and/or reduced radiation. Radiation treatment is associated with an increased risk of subsequent neoplasms in survivors of CNS malignancies, including gliomas and meningiomas. Radiation is not always needed for low-grade tumors.
vary depending on tumor type, location, and grade. While there has been progress in survival for Central Nervous System (CNS) tumors overall, there has been little progress for some subtypes, such as diffuse intrinsic pontine glioma (DIPG), for which the median survival time after diagnosis remains less than one year. Improvements in survival for many types of CNS malignancies have resulted from advances in neurosurgical techniques, delivery of radiation therapy, supportive care, and use of combination chemotherapy. Nevertheless, children treated for brain tumors have a high risk of long-term morbidity and mortality. Late neurologic complications observed in follow-up studies of 5-year survivors include new onset of seizures, weakness in the arms and legs, blindness, and hearing loss. Children who receive radiation therapy to the hypothalamic-pituitary axis often experience neuroendocrine effects, including growth hormone deficiency, hypothyroidism, and abnormal timing of menarche. Cranial radiation therapy, particularly when used in very young children, can also result in neurocognitive deficits. For this reason, treatment protocols for patients with CNS tumors have been modified so that children aged younger than 3 years usually receive chemotherapy first with delayed and/or reduced radiation. Radiation treatment is associated with an increased risk of subsequent neoplasms in survivors of CNS malignancies, including gliomas and meningiomas. Radiation is not always needed for low-grade tumors.
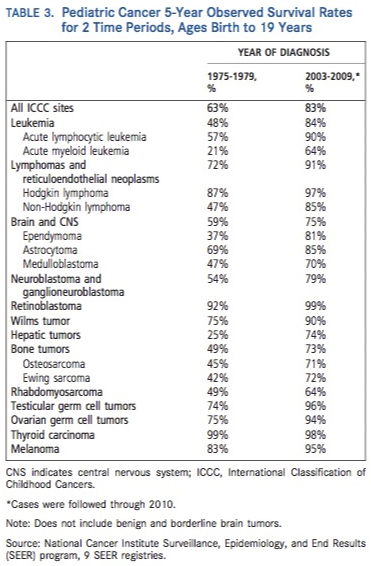
Neuroblastoma**: – Children who are treated for high-risk disease have the greatest risk of treatment-related complications, including severe sensorineural hearing loss, infertility, cardiac toxicity, and second neoplasms related to high-dose chemotherapy. Overall survival rates for children with neuroblastoma have increased from 54% between 1975 and 1979 to 79% between 2003 and 2009
Wilms Tumor**: Late effects observed among survivors of WT include kyphosis and scoliosis from radiation to the spine, anthracycline-related cardiotoxicity, end-stage renal failure, an increased risk of second malignancies, and infertility and pregnancy complications among girls treated with radiation. The risk of end-stage renal failure is increased among patients treated for bilateral disease and those receiving radiation to the opposite kidney in unilateral disease, as well as those with congenital syndromes and anomalies associated with the WT1 gene region.
Retinoblastoma**: Late effects of retinoblastoma include visual impairment and an increased risk of secondary neoplasms, including bone and soft tissue sarcomas and melanoma.
Osteosarcoma**: Therapy-related late effects can include anthracycline-induced cardiomyopathy, cisplatin-related hearing loss, kidney dysfunction, second malignancies, and infertility, especially in patients receiving alkylating agents. Patients treated for OS may have physical limitations resulting from surgical resection.
Ewing Sarcoma**: ES survivors are at increased risk of developing second cancers, cardiac and pulmonary conditions, infertility, and musculoskeletal problems.
Rhabdomyosarcoma**: Late effects of treatment for RMS vary depending on whether radiation therapy was given and the specific chemotherapy agents received, which have differed over time. Bones and soft tissues that get radiation do not grow very well. Depending on the area getting radiation, it may cause problems such as curvature of the spine, a shortened arm or leg, limited motion of a joint, hardening of the surrounding soft tissue, stiffening of the lungs, poor development of the facial bones, cataracts and poor vision of the involved eye, later problems with sexual function, and other problems. Young children’s brains are especially sensitive to radiation to the head, which can lead to learning problems or other issues, so doctors do their best to avoid this when possible. Second cancers are possible but only affect a small number of RMS survivors, and these are children who most likely would not have survived without these treatments. Treatments for patients with intermediate-risk and high-risk disease continue to be studied in clinical trials in the hopes of achieving better outcomes.
Ovarian Germ Cell Tumors**: The chemotherapy regimens most commonly used for OGC tumors may cause hearing loss and kidney toxicity.
Testicular Germ Cell Tumors**: Survival rates for testicular cancer have improved substantially since the mid-1970s (from 74% to 96% in 2003-2009), and most patients have a good prognosis.
 The most important action a childhood cancer survivor can take is to become totally engaged in their own healthcare. They should have a complete and detailed treatment summary or journal of all procedures (radiation, chemotherapy, drugs, etc.) completed during the time they were in cancer treatment. This is something that your cancer care facility should provide for you. The completed journal will be invaluable five, ten, fifteen, or more years down the road. Every primary care physician encountered along life’s path needs to have a copy of the journal and should demonstrate that they are aware of late-term side effects possible with past cancer treatments.
The most important action a childhood cancer survivor can take is to become totally engaged in their own healthcare. They should have a complete and detailed treatment summary or journal of all procedures (radiation, chemotherapy, drugs, etc.) completed during the time they were in cancer treatment. This is something that your cancer care facility should provide for you. The completed journal will be invaluable five, ten, fifteen, or more years down the road. Every primary care physician encountered along life’s path needs to have a copy of the journal and should demonstrate that they are aware of late-term side effects possible with past cancer treatments.
If your child is presently in cancer treatment now, talk to your oncologist or palliative care contact to ensure that you will have a complete record of all treatments.
Author: Joe Baber
** Source: American Cancer Society, Childhood and Adolescent Cancer Statistics, 2014 published in CA: A Cancer Journal for Clinicians, January 31, 2014.
Updated 6/1/2023



 panel discussions and presentations were unprecedented in my 6 years of advocacy experience. The opening night was a documentary on “progeria” that educated us about this disease that had no treatment. The documentary is a case study of how a single family rallied around this disease and pushed a drug through to market that is actually adding about 5 years to these kids life expectancy through drugs that improve their vascular strength.
panel discussions and presentations were unprecedented in my 6 years of advocacy experience. The opening night was a documentary on “progeria” that educated us about this disease that had no treatment. The documentary is a case study of how a single family rallied around this disease and pushed a drug through to market that is actually adding about 5 years to these kids life expectancy through drugs that improve their vascular strength.



 C is for Cancer Camp
C is for Cancer Camp


































 palliative care, and most health care professionals believe it is synonymous with end-of-life care.”
palliative care, and most health care professionals believe it is synonymous with end-of-life care.”