I am not sure how many people outside of the cancer research community know this, but it is well recognized that the human body is equipped to fight off cancer on its own. The same immune system that we have to fight infections should be able to fight off cancerous cells and tumors. While all cancers arise from an individual’s DNA damage and thus from our own cells, there are things about cancerous cells that are very unusual. Sometimes they express very high levels of certain types of proteins and other things which make them stand out from normal cells, and explains why they grow and progress as they do. Our immune system should be able to recognize such cells as foreign invaders and zap them before they become a problem. There is actually a theory, one which I happen to believe, that everybody develops cancer at various points in our lifetime, but that the tumors are eradicated by our immune system before we even know they are there. We all develop DNA damage, every single day, and so it makes sense that cancers come and go in uneventful fashion. Immune system activity is also a very logical explanation for why some patients will have an unexplained “spontaneous remission” in the absence of treatment. The immune system is likely behind such miracles.
 But 1 in 2 men, 1 in 3 women, and 1 in 285 children will get diagnosed with cancer, so we know that the immune system is not bullet proof. We know that patients who are in some way immunocompromised, such as patients who are undergoing immunosuppressive therapy because of an organ transplant or autoimmune condition and those with immunosuppressive conditions such as HIV/AIDS, have very elevated risks of developing cancer simply because they are immunosuppressed. But why does someone who is otherwise perfectly healthy, with no predisposition for cancer, get cancer? A deteriorating immune system with aging is thought to play a role in why cancer is so common in elderly patients, but to what extent does the immature immune system of childhood play a role in pediatric cancers? There are no clear answers to these questions, and the topic goes way beyond that of the immune system. However, we know more than we used to when it comes to the human immune system. Medical research has uncovered something really sneaky about tumors: that some tumors develop in ways that in essence get the immune system to look the other way. Unfortunately or fortunately, depending on your perspective, we now know that tumors are sometimes protected from the immune system via checkpoints like “PD1” (stands for programmed death-1; you may have heard of it, it is big news in cancer right now), leading to a new class of immunotherapy drugs called “checkpoint inhibitors”. Think of PD1 and other checkpoints (there are others, like CTLA-4, which was described before PD1) as being a brake to the immune system, telling the T-cells of our immune system to leave the cancer alone. We have these cellular checkpoints in our body to prevent our body from attacking itself (as happens in autoimmune diseases), but they are also offering protection to tumors. These new checkpoint inhibitor drugs are leading to major breakthroughs in advanced/metastatic melanoma, an aggressive skin cancer that had typically been considered a death sentence, usually within 1 year of diagnosis. In September 2014, the first PD1 checkpoint inhibitor was approved in the United States for advanced melanoma (Merck’s Keytruda® [generic is pembrolizumab so just call it Keytruda]); also another PD-1 agent, Bristol-Myers Squibb’s nivolumab (Opdivo®) has been approved for advanced melanoma in Japan and was just approved for use in the US by the FDA. Other similar agents are aggressively being explored as single-agent therapy and combination therapy melanoma and various other malignancies. The approval of Keytruda® was based on a 24% response rate in this heavily pretreated population in which most patients had stage IV metastatic disease, but even
But 1 in 2 men, 1 in 3 women, and 1 in 285 children will get diagnosed with cancer, so we know that the immune system is not bullet proof. We know that patients who are in some way immunocompromised, such as patients who are undergoing immunosuppressive therapy because of an organ transplant or autoimmune condition and those with immunosuppressive conditions such as HIV/AIDS, have very elevated risks of developing cancer simply because they are immunosuppressed. But why does someone who is otherwise perfectly healthy, with no predisposition for cancer, get cancer? A deteriorating immune system with aging is thought to play a role in why cancer is so common in elderly patients, but to what extent does the immature immune system of childhood play a role in pediatric cancers? There are no clear answers to these questions, and the topic goes way beyond that of the immune system. However, we know more than we used to when it comes to the human immune system. Medical research has uncovered something really sneaky about tumors: that some tumors develop in ways that in essence get the immune system to look the other way. Unfortunately or fortunately, depending on your perspective, we now know that tumors are sometimes protected from the immune system via checkpoints like “PD1” (stands for programmed death-1; you may have heard of it, it is big news in cancer right now), leading to a new class of immunotherapy drugs called “checkpoint inhibitors”. Think of PD1 and other checkpoints (there are others, like CTLA-4, which was described before PD1) as being a brake to the immune system, telling the T-cells of our immune system to leave the cancer alone. We have these cellular checkpoints in our body to prevent our body from attacking itself (as happens in autoimmune diseases), but they are also offering protection to tumors. These new checkpoint inhibitor drugs are leading to major breakthroughs in advanced/metastatic melanoma, an aggressive skin cancer that had typically been considered a death sentence, usually within 1 year of diagnosis. In September 2014, the first PD1 checkpoint inhibitor was approved in the United States for advanced melanoma (Merck’s Keytruda® [generic is pembrolizumab so just call it Keytruda]); also another PD-1 agent, Bristol-Myers Squibb’s nivolumab (Opdivo®) has been approved for advanced melanoma in Japan and was just approved for use in the US by the FDA. Other similar agents are aggressively being explored as single-agent therapy and combination therapy melanoma and various other malignancies. The approval of Keytruda® was based on a 24% response rate in this heavily pretreated population in which most patients had stage IV metastatic disease, but even  more noteworthy was that the responses tended to be durable in patients who responded. PD1 agents are not without side effects but are generally more tolerable than chemotherapy, producing mostly low-grade toxicity and not the types of things seen with chemotherapy. This is a big breakthrough for those whom chemotherapy has offered little hope but lots of toxicity.
more noteworthy was that the responses tended to be durable in patients who responded. PD1 agents are not without side effects but are generally more tolerable than chemotherapy, producing mostly low-grade toxicity and not the types of things seen with chemotherapy. This is a big breakthrough for those whom chemotherapy has offered little hope but lots of toxicity.
You might be thinking, why the upfront focus on advanced and metastatic melanoma for these new immunotherapies? Without getting into specifics regarding the biology of melanoma, there are things about melanoma that make it a very good target for immunotherapy, and is one of the cancers for which there has been some success with past attempts with older immunotherapy approaches, known as cytokines (the interleukins and interferons). So starting with advanced melanoma makes a whole lot of sense, from a biologic perspective. Anti-PD1 therapy is still in its infancy overall, but it is important for those reading this to know that pediatric studies of these PD1 agents are planned, per publically available information on the FDA’s website. The manufacturers of these products all recognize the potential of these agents for kids, and studies will be coming.
But the subject of PD1 immunotherapy will be continued at a later time, as it was not PD1 that prompted me to write this post. It is something else, called CAR T-cell therapy, for which pediatric data are already available.
Before I get into the data that have come to light for CAR T-cell immunotherapy for childhood leukemia, I think it is important to jump back and offer a little bit of context. I am an oncology writer who works as a contractor for the pharmaceutical/biotech industry. I have been writing about cancer drugs since 1998, and have witnessed the evolution of cancer therapy and the ups and downs with things like immunotherapy. In the early 2000s, cancer immunotherapy was the greatest thing since sliced bread. One of the big focus areas was therapeutic cancer vaccines. Unlike preventative vaccines (including those that are aimed at preventing cancer, like Gardasil), therapeutic cancer vaccines are designed to eradicate an existing cancer, by boosting the immune system as discussed earlier. In the early 2000s, several different therapeutic cancer vaccines were under development, including some complex personalized approaches that were based on the patient’s own unique cancer cells and others that were designed to be more “out-of-the-box”. Several showed promising early activity, but around the same time several different ones failed advanced-stage clinical trials. The populations that were mainly being studied were very heavily pretreated poor-prognosis cancers, like metastatic melanoma and advanced pancreatic cancer. Although many were speculating that these might not have been the best populations, that better results may have been possible if these vaccines had been tried earlier in the disease or in different types of tumors, many companies jumped off of the immunotherapy bandwagon entirely. Some small biotech companies, which were very dedicated to this therapeutic cancer vaccine technology, were forced to close their doors. I watched it happen. Some of these were my clients. My thought at that time was “Nooooooooo, don’t do it, stick with immunotherapy, we are on the right track but wrong train”. The concept of immunotherapy just makes sense on so many levels, and holds such promise for true cancer cures. But failed trials are an automatic death sentence for products, especially for small companies. Trying to manufacturer personalized cancer vaccines, a new and very complex and expensive process, just isn’t possible without money  and lots of it.
and lots of it.
So starting around the mid-2000s, things got very quiet on the immunotherapy front. Cancer became a bigger and bigger area for both large and small pharmaceutical/ biotech companies, but the focus wasn’t immunotherapy but something called targeted therapy. You may have heard terms like small-molecule inhibitors, molecularly targeted agents, tyrosine kinase inhibitors (TKIs), monoclonal antibodies — these terms all fall under the umbrella of the novel concept of targeting the ability of cancers to grow and proliferate by targeting cell survival pathways, rather than killing them directly via chemotherapy.
Chemotherapy basically works by causing damage to DNA, killing the tumors via this DNA damage (but unfortunately also damaging healthy DNA in the process). On the other hand, targeted agents work by indirect killing of the tumor, not by damaging its DNA but more like starving it by taking away something(s) that it should need to survive. As I mentioned earlier, cancers express high levels of things that normal cells express at low levels, so modern medicine has been able to exploit those differences and develop these new “targeted agents” that represent “personalized medicine”. However, the term “targeted” is kind of a misnomer. For example, there is a modern class of drugs called EGFR inhibitors, which act against tumors that have identifiable mutations in this thing called EGFR. EGFR mutations commonly occur in certain patients including non-smokers with lung cancer, and these EGFR-targeted agents are being used as a substitute for chemotherapy in these patients. These agents are way more effective than chemotherapy in these patients, assuming that the patient has a tumor that carries an EGFR mutation (this is where genomic profiling comes into play, to be discussed another time), and more tolerable to
 boot. However, they are not devoid of toxicity. For example, EGFR is highly expressed in normal skin, so these “targeted agents” can lead to skin toxicity, which can be severe and complicate treatment. So the term targeted does not mean that the activity of these drugs is confined to the tumor per se. At the same time, however, these drugs are NOT chemotherapy and generally do not produce the types of severe toxicity commonly seen with chemotherapy, and many of them are available as once-daily oral therapy which is a welcome convenience. Overall, molecular targeted therapy is a good thing and represents a huge leap forward in cancer therapy. It has revolutionized the entire approach to treatment, allowing for a personalized approach that can lead to better efficacy and better tolerability. However, a big barrier to targeted therapy is tumor resistance, either at the start of treatment or after a while of being on treatment. As I said earlier, tumors are sneaky. If you block a cell survival pathway (like EGFR or something else, there are many!), tumors can find ways to eventually adapt and grow without that particular pathway. Tumor resistance is considered inevitable for most patients treated with targeted therapy, although some patients will continue to respond over time. Researchers are still trying to figure out ways to stop this resistance, such as by combining agents. Sometimes this seems to work; other times, not so much. Always remember, every single solitary tumor is unique, being derived by our own DNA. This explains why patient experiences and outcomes vary so much.
boot. However, they are not devoid of toxicity. For example, EGFR is highly expressed in normal skin, so these “targeted agents” can lead to skin toxicity, which can be severe and complicate treatment. So the term targeted does not mean that the activity of these drugs is confined to the tumor per se. At the same time, however, these drugs are NOT chemotherapy and generally do not produce the types of severe toxicity commonly seen with chemotherapy, and many of them are available as once-daily oral therapy which is a welcome convenience. Overall, molecular targeted therapy is a good thing and represents a huge leap forward in cancer therapy. It has revolutionized the entire approach to treatment, allowing for a personalized approach that can lead to better efficacy and better tolerability. However, a big barrier to targeted therapy is tumor resistance, either at the start of treatment or after a while of being on treatment. As I said earlier, tumors are sneaky. If you block a cell survival pathway (like EGFR or something else, there are many!), tumors can find ways to eventually adapt and grow without that particular pathway. Tumor resistance is considered inevitable for most patients treated with targeted therapy, although some patients will continue to respond over time. Researchers are still trying to figure out ways to stop this resistance, such as by combining agents. Sometimes this seems to work; other times, not so much. Always remember, every single solitary tumor is unique, being derived by our own DNA. This explains why patient experiences and outcomes vary so much.
Meanwhile, as the pharmaceutical/biotech progress was being made with targeted agents, the field of immunotherapy was not entirely dead, as illustrated by the PD1 example earlier. At the University of Pennsylvania, researchers were focusing on an entirely different type of cancer immunotherapy, termed CAR (chimeric antigen receptor) T-cell therapy. Our immune system is composed of a mixture of T-cells and B-cells, which act in different ways to fight infections and other invaders. The concept here is that you take T-cells from a patient, send them to a lab and use a virus to genetically program the native T-cells to target cancer cells, and re-inject them into the patient in hopes that these “serial killer cells” will do their thing and knock off the cancer. On a fascinating note, the reprogramming is taking place via use of the HIV virus, which is a very effective means of delivering information to T-cells. The HIV virus is of course deactivated so that it cannot
 cause disease. As it turns out, these serial killer cells are actually doing their thing. Not only are we seeing positive results, but a focus to date has been treatment-refractory pediatric acute lymphoblastic leukemia (ALL)!! Check out this video, “Fire With Fire”, but be prepared to be blown away:
cause disease. As it turns out, these serial killer cells are actually doing their thing. Not only are we seeing positive results, but a focus to date has been treatment-refractory pediatric acute lymphoblastic leukemia (ALL)!! Check out this video, “Fire With Fire”, but be prepared to be blown away:
The experiences with CAR T-cell therapy have been published in the New England Journal of Medicine, based on a study conducted at the Children’s Hospital of Philadelphia (CHOP).1,2 The first report described the first 2 patients achieving complete remission, whereas the most recent one reported a 90% complete response rate among 30 children or adults with relapsed or refractory ALL, with some durable remissions up to 24 months. Recently, updated data were reported at the Annual Meeting of the American Society of Hematology, with a 92% complete remission rate among 39 children and young adults. Results like this, in such heavily pretreated patients with no other treatment options and such a poor prognosis, are pretty much unprecedented. CAR T-cell therapy is not without toxicity issues. Because you are boosting the immune system so strongly, all patients experience something called cytokine-release syndrome, which can lead to life-threatening complications. The “serial  killer cells” also kill healthy B-cells in the process, requiring patients to receive B-cell replacement therapy indefinitely. Also, this particular therapy is targeted against CD19, a certain tumor marker that is not expressed in all ALL. Finally, as explained by Dr. Stephen Grupp from CHOP in the video to the right, patients who are so heavily pretreated have a risk of not having enough T-cells to do this type of therapy. It begs the question, of just how early something like this could be tried? And what will the long-term results be, in terms of “immunity” against recurrence? Answers to questions like that will take further studies, and a multicenter study for pediatric ALL is already planned (yay!).
killer cells” also kill healthy B-cells in the process, requiring patients to receive B-cell replacement therapy indefinitely. Also, this particular therapy is targeted against CD19, a certain tumor marker that is not expressed in all ALL. Finally, as explained by Dr. Stephen Grupp from CHOP in the video to the right, patients who are so heavily pretreated have a risk of not having enough T-cells to do this type of therapy. It begs the question, of just how early something like this could be tried? And what will the long-term results be, in terms of “immunity” against recurrence? Answers to questions like that will take further studies, and a multicenter study for pediatric ALL is already planned (yay!).  Also, because of the excitement around this product, it really resonated with the pharmaceutical/biotech industry, with the University of Pennsylvania’s technology being licensed by Novartis Pharmaceuticals. Novartis is working on building a manufacturing facility to facilitate the expansion of this therapy within the United States and abroad. Other companies have ventured into the CAR T-cell space. This is a huge deal and speaks volumes to the promise for this technology, as this type of personalized product is not the typical type of treatment for large companies to take on.
Also, because of the excitement around this product, it really resonated with the pharmaceutical/biotech industry, with the University of Pennsylvania’s technology being licensed by Novartis Pharmaceuticals. Novartis is working on building a manufacturing facility to facilitate the expansion of this therapy within the United States and abroad. Other companies have ventured into the CAR T-cell space. This is a huge deal and speaks volumes to the promise for this technology, as this type of personalized product is not the typical type of treatment for large companies to take on.

Click here for more on this article
This type of technology is very complex and requires a lot of money and patience, to keep it alive. Research hospitals, even major ones like UPenn/CHOP, certainly cannot go down this road alone, so it is a good thing for everyone that pharma came knocking. It took some time to generate interest. It took groundbreaking results, but CAR T-cell therapy found the home it needs to take it to the next level.
So right now, everybody in the cancer world is talking about immunotherapy as the greatest thing since sliced bread. I tend to agree. We have a long road ahead though. The experience with CAR T-cell therapy has been so positive so far, but responses like that will not be achieved for every patient in every trial. Long-term efficacy and safety data are critical, but that takes time. Nonetheless–immunotherapy is BACK and seemingly here to stay, and I am personally so excited to see what’s next. I follow this area of immunotherapy very closely, not just for children but for adults, and I will be sure to keep you posted too!
Author: Laurie Orloski
References:
- Maude SL, Frey N, Shaw PA, et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N Engl J Med. 2014 Oct 16;371(16):1507-17.
- Grupp SA, Kalos M, Barrett D, et al. Chimeric antigen receptor-modified T cells for acute lymphoid leukemia. N Engl J Med. 2013 Apr 18;368(16):1509-18.



 The other day I decided to take my 7 year old daughter, Bella, out on a date. I found a traveling circus that was in town and recalled how much I enjoyed the circus as a kid and thought it would be a great opportunity to make some memories with my little princess. On the way I asked her to choose what she wanted for dinner and that we were in a hurry so it couldn’t be somewhere that takes too long. She choose Dairy Queen for some unknown reason? Ya right, she couldn’t wait until after she ate her burger for her ice cream. Then I remembered since it was a date, I shouldn’t be scolding her about eating her ice cream first. Shortly after getting back in the car she asked “how did Caleb die?”
The other day I decided to take my 7 year old daughter, Bella, out on a date. I found a traveling circus that was in town and recalled how much I enjoyed the circus as a kid and thought it would be a great opportunity to make some memories with my little princess. On the way I asked her to choose what she wanted for dinner and that we were in a hurry so it couldn’t be somewhere that takes too long. She choose Dairy Queen for some unknown reason? Ya right, she couldn’t wait until after she ate her burger for her ice cream. Then I remembered since it was a date, I shouldn’t be scolding her about eating her ice cream first. Shortly after getting back in the car she asked “how did Caleb die?” You see, Bella doesn’t remember her only brother. Caleb was diagnosed with a rare form of Leukemia that sadly took him away just after his 4th birthday when Bella was only 9 months old. After the question sunk in, I asked her why she wanted to know how Caleb died. She said “because he was my brudder”. Touche’ I thought. Then I asked what she wanted to know? She knows he died of Leukemia. She said “what happened to him to make him die?” I asked do you mean what happened inside of his body? She exclaimed “Yes.”
You see, Bella doesn’t remember her only brother. Caleb was diagnosed with a rare form of Leukemia that sadly took him away just after his 4th birthday when Bella was only 9 months old. After the question sunk in, I asked her why she wanted to know how Caleb died. She said “because he was my brudder”. Touche’ I thought. Then I asked what she wanted to know? She knows he died of Leukemia. She said “what happened to him to make him die?” I asked do you mean what happened inside of his body? She exclaimed “Yes.” breathing and was gone to heaven.” She said “that’s very sad and I wish I was older so I could remember my big brudder.”
breathing and was gone to heaven.” She said “that’s very sad and I wish I was older so I could remember my big brudder.”

 When a patient achieves that magical 5 year survival mark, everyone celebrates the milestone and they are considered by most people to be “cured.” That is not necessarily accurate. What it means is exactly what it implies: They have survived five years since being diagnosed, nothing more. The average age at diagnosis of cancer is 6 for children and 66 for adults. While the chart at the right shows great progress has been made in five year survival rates in childhood cancer over the last 40 years, it is only comparing five year survival rates, nothing more. While it gives some comfort that we appear to be making good progress, it does not really measure survival
When a patient achieves that magical 5 year survival mark, everyone celebrates the milestone and they are considered by most people to be “cured.” That is not necessarily accurate. What it means is exactly what it implies: They have survived five years since being diagnosed, nothing more. The average age at diagnosis of cancer is 6 for children and 66 for adults. While the chart at the right shows great progress has been made in five year survival rates in childhood cancer over the last 40 years, it is only comparing five year survival rates, nothing more. While it gives some comfort that we appear to be making good progress, it does not really measure survival 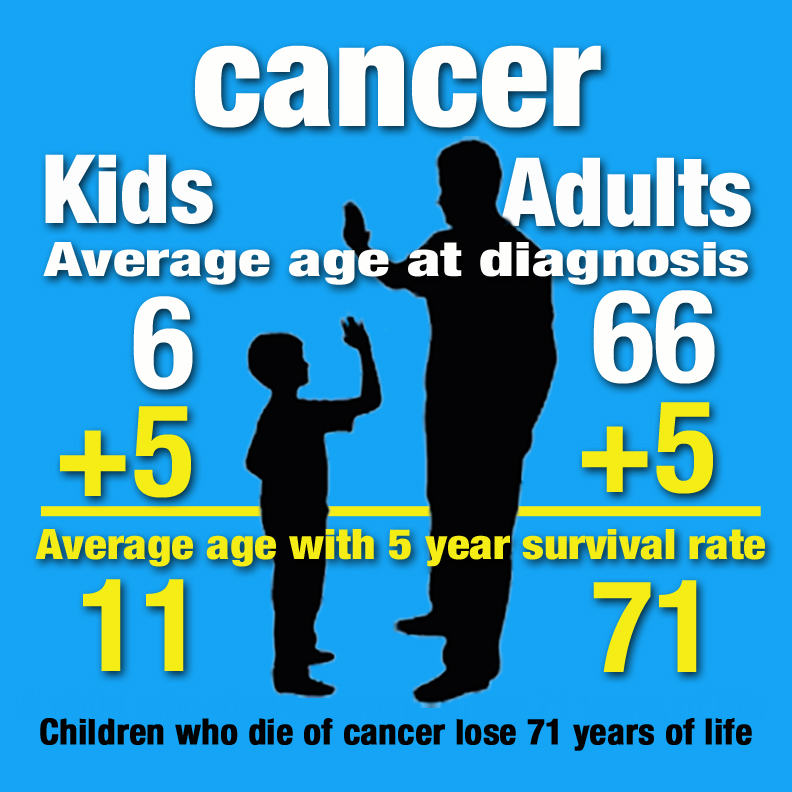























































 When we first announced the name of our foundation, people thought we were a little crazy. I understand that the name is unconventional, but so is our goal. It is different. Some might say impossible. So our name reflects not only the enormity of the task, but also that we plan to be successful.
When we first announced the name of our foundation, people thought we were a little crazy. I understand that the name is unconventional, but so is our goal. It is different. Some might say impossible. So our name reflects not only the enormity of the task, but also that we plan to be successful.






 The model of care at Ladybug House will be holistic, integrative, and life-promoting; these elements together will create a health-enhancing cooperative effect for patients as well as their families and friends.
The model of care at Ladybug House will be holistic, integrative, and life-promoting; these elements together will create a health-enhancing cooperative effect for patients as well as their families and friends.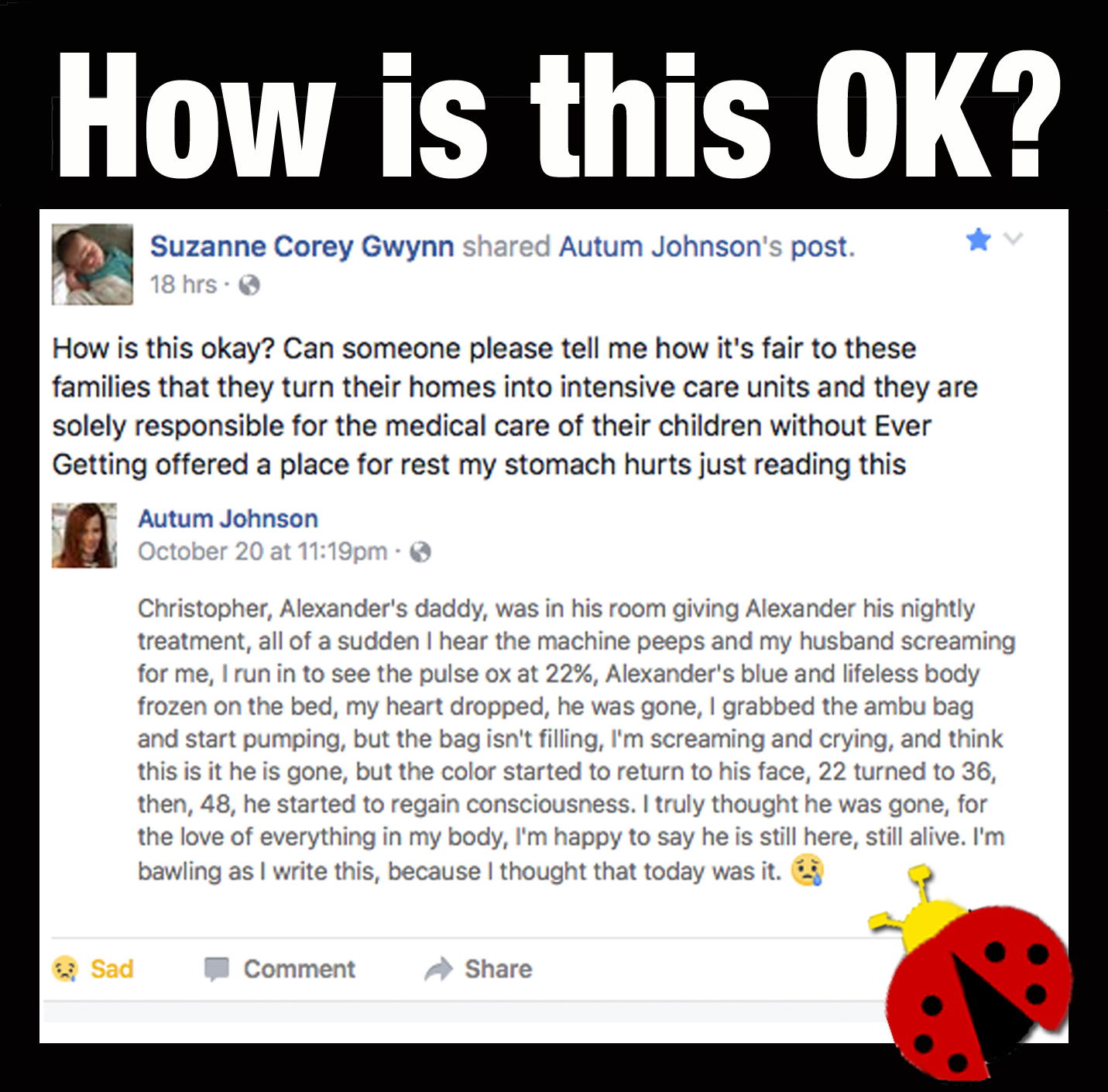
 Editor’s Note: Because of her efforts and the unique home she plans to build, Suzanne was invited to the White House on June 18, 2014 where she was able to collaborate with others and garner more support for her vision.
Editor’s Note: Because of her efforts and the unique home she plans to build, Suzanne was invited to the White House on June 18, 2014 where she was able to collaborate with others and garner more support for her vision.

 A Critical Circle of Family Support
A Critical Circle of Family Support
 Terminally Ill Kids Need Different Care Than Adults
Terminally Ill Kids Need Different Care Than Adults






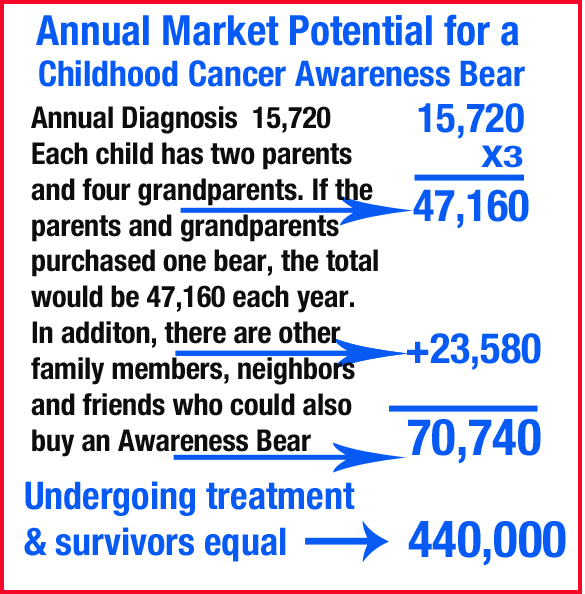
 During my time as a nurse, I discovered several truths: (1) Many people are not aware of the large number of children being diagnosed with cancer until they have a child that receives the awful, and surprising diagnosis. Today, each and everyday, 46 children will be diagnosed with cancer. (2) Childhood cancer is not as rare as most people think it is. Worldwide, over 300,000 children will get cancer each year. Many children are being diagnosed with thyroid, kidney, and brain cancers that were formally known as “adult cancers.
During my time as a nurse, I discovered several truths: (1) Many people are not aware of the large number of children being diagnosed with cancer until they have a child that receives the awful, and surprising diagnosis. Today, each and everyday, 46 children will be diagnosed with cancer. (2) Childhood cancer is not as rare as most people think it is. Worldwide, over 300,000 children will get cancer each year. Many children are being diagnosed with thyroid, kidney, and brain cancers that were formally known as “adult cancers.